INTRODUCTION
Bronchogenic Cysts
should be considered in the evaluation of mediastinal
lesions. These embryologic remnants occur
as developmental abnormalities of the primitive foregut. Bronchogenic Cysts
may present with compressive symptoms such as chest pain, cough, dyspnea, or acute respiratory distress particularly in
children.1 In the
absence of adjacent structures prone to compression most bronchogenic
cysts remain asymptomatic.2 The following case report describes
our experience with an asymptomatic Bronchogenic
Cyst.
CASE REPORT
A 29 year old female
underwent preoperative evaluation for anterior lumbar interbody
fusion. Chest x-ray revealed a poorly
localized right sided paravertebral lesion. The patient denied any significant
symptoms. Specifically, she denied chest
pain, dyspnea, cough, fever, chills, smoking history
or exposure to TB. The patient’s past
medical history included: lumbar disc herniation,
appendectomy, and tonsillectomy. The physical exam was unremarkable with lungs
clear on auscultation.
The screening chest x-ray taken in February 2002
revealed a right sided 4 cm round density on lateral view. The density was overlying the lower thoracic
vertebrae. The lesion was further
evaluated with CT scan with intravenous contrast, revealing a 3.8 x 2.7 cm
right paraspinal mass at the level of T 10. There were no associated pleural effusions or
lymphadenopathy.
Possible differential diagnosis included: a schwanoma,
neurofibroma, ganglioneuroma
and paraganglioneuroma.
A chest CT scan was repeated approximately six months
later. The patient remained asymptomatic and the CT scan was unchanged. A fibreoptic bronchoscopy with exploratory right video assisted thoracic
surgery was performed for presumed neurogenic
tumor.
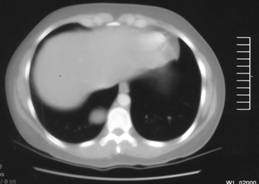
Figure-1:
CT scan with intravenous contrast revealed a 3.8 x 2.7 cm right paraspinal mass at the level of T10.
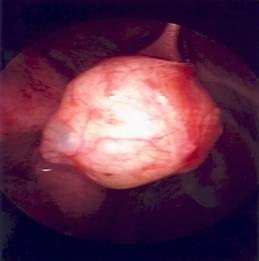
Figure-2:
Appearance on bronchoscopy
The
tumor was visualized after retracting the diaphragm inferiorly and the lung
superiorly. The tumor was tethered by a
narrow stalk, which was isolated and divided.
The specimen was sent to pathology.
On gross examination, the mass was described as a cystic lesion filled
with mucoid thick viscous fluid within a rubbery ring
like structure. On frozen section the
cyst was lined with bronchial epithelium establishing the diagnosis of a Bronchogenic Cyst.
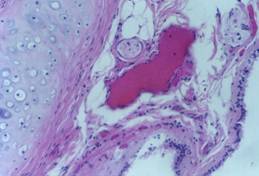
Figure-3:
Histological Appearance
DISCUSSION
Most Bronchogenic Cysts are found in the mediastinum
reflecting their embryologic origin from the primitive foregut.3
Since
Bronchogenic Cysts are derived from the tracheobronchial tree, there is
often an attachment/stalk as seen in our patient. Increasingly VATS is used preferentially over
an open technique for resection. Martinod et al. were able to excise 65% of the Bronchogenic Cysts via thoracoscopy.4 Interestingly
neither size nor mediastinal location were the
determining factors for successful thoracoscopic
resection. Rather, the presence of
adhesions and vascular complications determined the need for the more
traditional thoracotomy approach. Laparoscopic resection is preferred due to
reduction in length of hospital stay and the reduction in postoperative
pain.
The majority of Bronchogenic
Cysts remain asymptomatic. Consequently some argue that treatment of Bronchogenic Cysts is controversial. Due to the difficulty
in preoperative diagnosis, the lesions are treated surgically by enucleation. However, Bronchogenic
Cysts are known to undergo malignant transformation into carcinomas and
sarcomas. Also they are known to become infected and may fluctuate in size
causing compressive symptoms. There are reports of acute respiratory distress in
pediatric patients attributed to Bronchogenic Cysts
secondary to their mediastinal location.5 Clearly
such patients require urgent surgical intervention.
The role of MRI and TEE in the evaluation of Bronchogenic Cysts has been investigated by
In
conclusion, the diagnosis of Bronchogenic Cyst
ultimately depends on the histopathological diagnosis
confirming the presence of respiratory epithelium in the resected
mass. Thoracoscopic resection of Bronchogenic
Cysts is a viable surgical option for the removal of uncomplicated lesions.
REFERENCES
1.
Ribet
ME, Copin MC, Gosselin B. Bronchogenic cysts of the mediastinum.
J Thorac Cardiovasc Surg 1995;109:1003-10
2.
Coselli MP, de Ipolyi P, Bloss RS, Diaz RF,
Fitzgerald JB. Bronchogenic cysts above
and below the diaphragm: report of eight cases. Ann Thorac
Surg 1987;44(5):491-4.
3.
Ingu A, Watanabe A, Ichimiya Y, Saito T, Abe T. Retroperitoneal bronchogenic cyst: a case report.
Chest 2002;121(4):1357-9.
4.
Martinod E, Pons F, Azorin J, Mouroux J, Dahan M, Faillon JM et al. Thoracoscopic
excision of mediastinal bronchogenic
cysts: results in 20 cases. Ann Thorac Surg 2000;69(5):1525-8
5.
Ahrens B, Wit J, Schmitt
M, Wahn U, Niggemann B,
Paul K. Symptomatic bronchogenic cyst in a six month
old infant: case report and review of the literature. J Thorac
Cardiovasc Surg 2001;122(5):1021-3
6.
Lugo-Olivieri CH, Schwartzman GJ, Beall
DP, Lima JA, Fishman EK. Intrapericardial bronchogenic cyst: assessment with magnetic resonance
imaging and transesophageal echocardiography. Clin Imaging 1999;23(2):81-4