Introduction
Strongyloides
stercoralis is a nematode that infests the human intestine especially in
tropical and subtropical regions, most of these infections being asymptomatic. However, it can cause substantial intestinal
disease and can disseminate widely to extra intestinal sites such as lungs,
kidney or brain (the hyper infection syndrome),
especially in the immunocompromised host1. In immunocompetent hosts,
these parasites cause a low grade, chronic infection, which has been seen even
up to 40 years after exposure2.
Presentation as malabsorption in an immunocompetent host is an uncommon
event. We report a case of a 55-year-old
immunocompetent male who presented with features of malabsorption because of
strongyloides stercoralis infestation.
Case History
A
55-year-old male labourer from
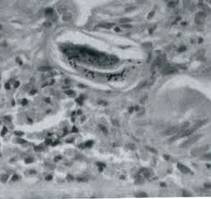
Fig-1: Strongyloides stercoralis larvae
(arrow) infiltrating the crypt
epithelium (H&E x 40)
He was treated with albendazole 10mg/kg/day for three
days but the stool examination done after seven days showed the persistence of
larvae. He was treated again with
Thiobendazole 25 mg/kg/day for three days.
Repeat stool examination done after one week was negative for the
larvae. On follow-up his diarrhoea had subsided and he
had started gaining weight.
Discussion
Strongyloidiasis
primarily presents with dermatological and gastroenterological (GI)
disease. Skin manifestations are usually
in the form of urticarial eruptions or ‘larva currens.’ None of these were
present in our patient. GI
manifestations are usually in the form of indigestion, cramping lower abdominal
pain, pruritis ani and intermittent or persistent dirrhoea.3 Various
uncommon GI manifestations have also been described,3 malabsorption
being one of them.4 Our patient had malabsorption as was evident on
characteristic history, physical examination, abnormal D-Xylose test and
findings on barium meal follow through examination. Strongyloides stercoralis
infestation was demonstrated by the presence of larvae in the stool and
endoscopic biopsies.
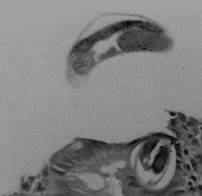
Fig-2:
Strongyloides stercoralis larvae, seen in the intestinal crypt epithelium in D2
biopsy, in an immunocompetent patient with malabsorption. The patient responded
to therapy with thiobendazole.
In most of the earlier reports of Strongyloidiasis,
patients presenting as chronic diarrhoea or malabsorption had either an
associated immunosuppressive illness or were on immunosuppressive treatment.5
In patients, who did not have any associated immunosuppressive disease or
medication, HIV was not excluded, it being a pre HIV era.5 Our
patient did not have any associated illness suggestive of immunosuppression and
was not on any immunosuppressive treatment.
He did not have history suggestive of congenital immune deficiency, and
had normal cell counts, normal serum globulins, a positive mantoux test and a
negative HIV serology.
Malabsorption in an immunocompetent patient because of
strongyloides stercoralis is an unusual manifestation and that makes this
case interesting.
References
1.
Gotuzzo E,
Terashima A, Alvarez H. Strongyloides stercoralis hyper infection associated
with human T cell lymphotrophic virus type I infection in
2.
Gill GV, Bell DR.
Strongyloides stercoralis infection in former far East prisoners of war. Br Med
J 1979; 2:572-4.
3.
Grove DI.
Strongyloidiasis: A conundrum for gastroenterologist. Gut 1994; 35:437-40.
4.
O’Brien W.
Intestinal malabsorption in an acute infection with Strongyloides stercoralis.
Trans R Soc Trop Med Hyg 1989; 150:92-3.
5.
Milder JE, Walzer
PD, Kilgore G, Rutherford I and Klein M. Clinical features of Strongyloides
stercoralis infection in an endemic area of the